E-Learning: 5th International CRAFTA® Congress (Kursbeschreibung)
Online (übrige Standorte ausblenden)

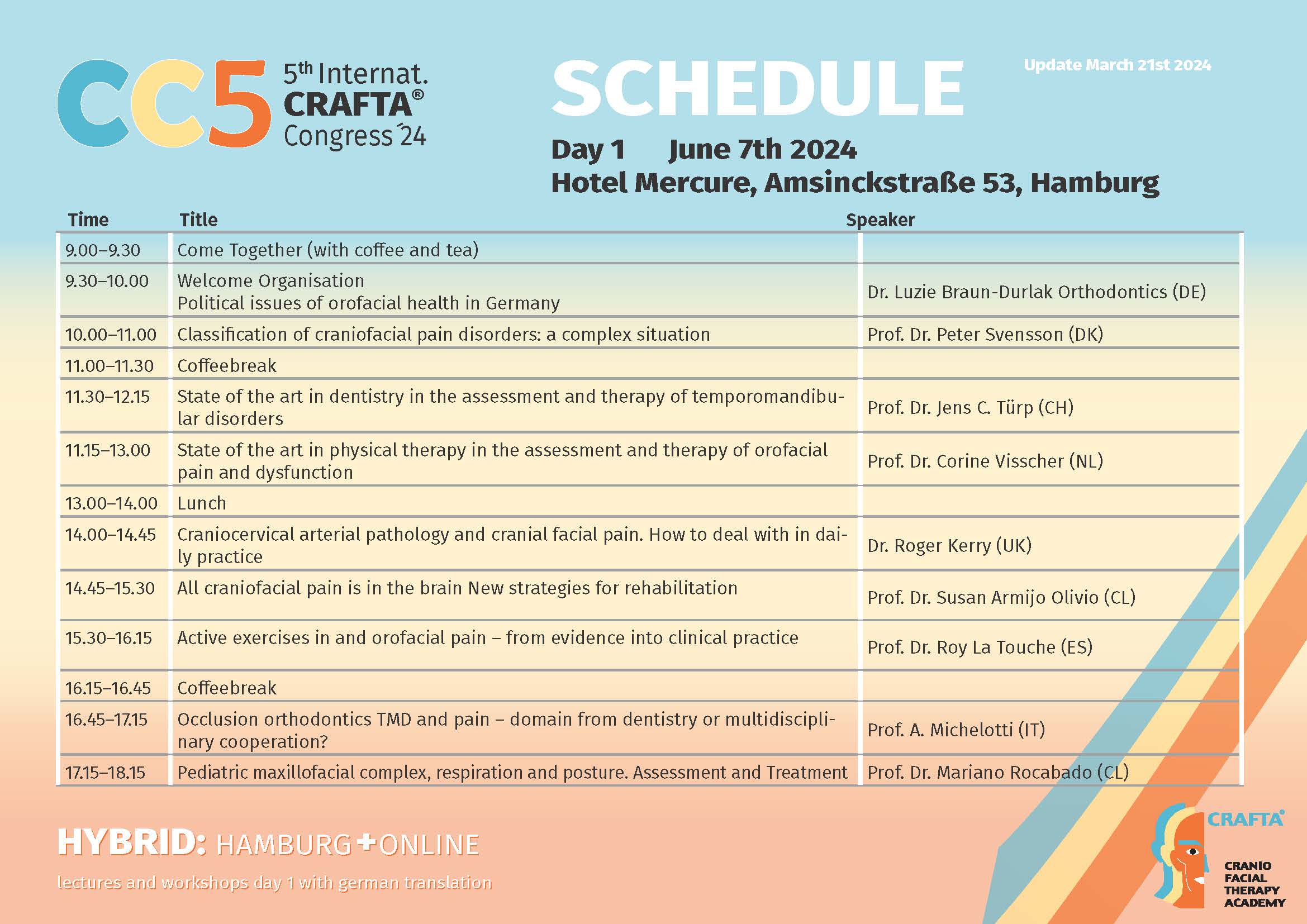
Political issues of orofacial health in Germany
Dr. med. dent. Luzie Braun-Durlak
In these days of the congress the urgently needed communication and exchange between dentists and pyhsiotherapists will actually take place. How can we organize in our daily routine and practices to continue this holistic, interdisciplinary cooperation and how can we support this politically by improving the conditions for treatment and communication?
Classification of craniofacial pain disorders: a complex situation
Prof. Dr. Peter Svensson, DDS, PhD, Dr.Odont
Classification of pain has greatly developed over the last couple of decades, in particular the recent International Association for the Study of Pain (IASP) and International Classification of Diseases (ICD-11) description of chronic pain as a disease or disorder in its own right (primary pain) is a game changer and clearly note the difference to pain as merely a symptom (secondary pain) (Treede et al. 2019). The International Classification of Headache Disorders (ICHD 2018) is another prominent and important classification system but looks at orofacial pains as secondary headaches attributed to various disorders in specific tissues. Temporomandibular Disorders (TMD) is the second most prevalent orofacial pain condition after odontogenic pains and has progressed substantially with the Research Diagnostic Criteria for TMD (RDC/TMD) (Dworkin and LeResche 1992) and the Diagnostic Criteria for TMD (DC/TMD) (Schiffman et al. 2014). The strengths of these classifications are operationalized criteria and known reproducibility and validity and the international adoption of a common approach to examine and diagnose both painful and non-painful orofacial musculoskeletal disorders. The limitations are obviously the lack of inclusion of other types of orofacial pain but the International Classification of Orofacial Pain (ICOP 2020) attempted to provide a comprehensive classification system of all types of acute and chronic orofacial pain based on the experience from RDC/TMD, DC/TMD, ICHD-3 and IASP-ICD11classifications. The talk will summarize the development of orofacial pain classification with a focus on the need to better integrate neck / cervical pain in future classification systems. This is not just an academic exercise but based on the intimate clinical and neurobiological relationships between some types of orofacial pains and neck / cervical pains leading to the discussion of the term “craniofacial pain” and how to proceed?
State of the art in dentistry in the assessment and therapy of TMDs
Prof. Dr. Jens Christoph Türp, DDS, Dr Med Dent, MSc, M.A.
A century ago, the German university professor Adolf von Strümpell pointed out that therapeutic agents can generally be classified hierarchically into four quality levels: necessary,
useful, unnecessary, and harmful (Dtsch Med Wochenschr 1922;48:1-5). Obviously, necessary therapies are the first choice. Depending on the case, they may be supplemented by useful
measures. It is clear that von Strümpell's classification can also be helpful in evaluating the quality of diagnostic procedures. My presentation will use this framework to address the question of which diagnostic and therapeutic interventions are necessary or useful for patients with temporomandibular
disorders (TMDs) – and which are unnecessary or even harmful. Relevant literature will be cited, such as the recently updated AAOP Guidelines for Assessment, Diagnosis, and Management of Orofacial Pain (2023). Of course, the role of physical therapy will also be addressed.
State of the art in physical therapy in the assessment and therapy of orofacial pain and dysfunction
Prof. Dr. Corine Visscher, BSc, MSc, PhD, PT
State of the art in physical therapy in the assessment and therapy of orofacial pain and dysfunction.
In this lecture, recent developments in the assessment of orofacial pain and dysfunction will be presented and discussed from an orofacial physical therapy point of view. The recently published brief Diagnostic Criteria for Temporomandibular Disorders (DC/TMD) will be covered, as well as the adaptation of the DC/TMD for its use in children and adolescents. In addition, the role of some frequently occurring types of headache, i.e. migraine and tension type headache, is discussed as part of the management of patients with orofacial pain. In this light, dr. Visscher will also present data on the prevalence of the less commonly diagnosed ‘headache associated with a TMD’ and she will pledge for a better recognition of this type of headache. Furthermore, a clinical reasoning strategy for orofacial pain and dysfunction is presented, embedding both psychosocial and physical symptoms as drivers for treatment options. Based
on the so-called axis I (physical) and axis II (psychosocial) symptoms, guidelines for mono- or multidisciplinary treatment are given. Pain education as treatment option will be highlighted in more detail. Last but not least, recent outcomes on the patient’s perspectives and the role of the physical therapist as part of the patient journey will be presented. Prof. dr. Corine Visscher, orofacial physical therapist (not practicing), director of the dental school (Academic Centre for Dentistry Amsterdam) and vice-president of the INFORM network.
Craniocervical arterial pathology and cranial facial pain. How to deal with in daily practice
Prof. Dr. Roger Kerry, BSc, MSc, PhD, PT
This talk will allow delegates to further enhance their understanding of screening and assessing for vascular causes of neck, head, and orofacial pain and dysfunction (Hutting et al, 2023). The talk will be based on the 2022 IFOMPT framework for examination of the cervical region for vascular pathologies (Rushton et al, 2022). A key premise for the talk is that vascular pathologies and dysfunctions have the potential to masquerade as neur0meuculoskeltal disorders, and as such, differential diagnosis is not straightforward. The talk will, therefore, set out a structure for best practice helping the clinician to recognise subtle but important signs and symptoms suggestive of serious vascular pathology (e.g. stroke) or anatomical dysfunction (e.g. Bow Hunter’s Syndrome).
Background data about risk, epidemiology, prognosis and screening will be presented before a focus on key pathophysiological matters, allowing the clinician to deepen their understanding of vascular pathology and support their clinical reasoning. This is information will then be translated into history taking and physical examination, equipping he clinician with the knowledge, skills, and confidence needed to assess and screen for vascular causes of pain. Short cases studies will be used to highlight key clinical messages and the delegates will be signposted to useful supporting resources.
Craniofacial pain and the brain: New strategies for rehabilitation
Prof. Dr. Susan Armijo Olivo, BSc, MSc, PhD, PT
Background: People with craniofacial pain and especially those with chronic
Temporomandibular disorders (TMDs) commonly have persistent pain, allodynia, and
hyperalgesia, sometimes extending to regions distant from the head, face, and neck regions. These patients demonstrate an abnormal function of the central nervous system similar to other
chronic painful conditions, especially those related to the musculoskeletal (MSK) system.
Cognitive and motor dysfunction have also been observed in this population that could be
related to abnormal activity of associated brain regions.
In recent years, abundant evidence from brain imaging techniques has shown that individuals
with musculoskeletal disorders (MSKDs) and pain (including people with craniofacial pain/TMDs) present with abnormal brain characteristics. Imaging studies specifically in individuals with craniofacial pain show alterations in several key regions in the brain. These brain alterations appear in brain structure (grey/white matter density and thickness as well as function (changes in blood oxygenation level dependent [BOLD] response).
In the last decade, several treatment approaches have been tested to target these alterations.
The evidence is still incipient in this field, but it is rapidly growing. Objective: The objective of this presentation is to highlight these findings as well as provide some insights into how to approach the treatment of these complex patients, especially those with craniofacial pain. Methods: Integration of the available literature with findings from studies conducted by our research team will be provided. The presentation will provide several different approaches to manage craniofacial pain using innovative and up to date strategies based on the current evidence. In particular, some preliminary results of a triple blind, two-armed parallel group, placebo-controlled pilot randomized controlled trial (RCT) investigating the effects of neck motor control training using visual feedback (MCTF) compared to placebo will be presented. In this study women with chronic jaw pain were randomized to receive an 8-week exercise
program consisting of neck exercises. Patients in the control group received a placebo
intervention using an innocuous electrical therapy called “TENS” (transcutaneous electrical nerve stimulation). Brain activity was measured at the beginning of the study and at the end
of the interventions (8 weeks). Participants also were asked about their pain, disability, and
psychological status at baseline, end of the treatment, and after 6 months of being randomized.
The effectiveness of motor control exercises on clinical as well as brain outcomes is being
analyzed. A discussion of possible effects of physical therapy strategies to target not only clinical but also brain abnormalities will be presented.
Active exercises in orofacial pain - from evidence into clinical practice
Prof. Dr. Alba Paris-Alemany, MD, PT, PhD
The objective of this presentation is to provide a structured and well-founded theoretical framework on the bio-behavioral characteristics of patients with craniofacial pain, analyzing how these characteristics impact disability and functional capacity. Additionally, we will explore the scientific evidence supporting the effectiveness of exercise prescription and other active treatments in patients with temporomandibular disorders and migraines and discuss strategies for their effective clinical implementation. Craniofacial pain, which can manifest as either acute or chronic, impacts various structures such as the temporomandibular joint and cranial and facial areas. This type of pain may be mediated by both peripheral and central mechanisms and encompasses conditions like migraines, craniofacial neuropathies, and temporomandibular disorders. Clinical symptoms can range from limitations in cranio-mandibular movement to masticatory fatigue and pain during orofacial activities, significantly increasing the level of disability in affected individuals. Additionally, patients with migraines often experience notable
reductions in physical activity levels and exhibit psychological issues such as kinesiophobia,
which further impair functionality. Therapeutic exercise has proven to be an effective clinical intervention that enhances functional capacity, reduces disability and pain intensity, and improves quality of life in these patients. An international consensus of experts advocates for the use of exercise as a beneficial treatment for patients experiencing mandibular function dysfunctions. Recent studies have shown that patients with temporomandibular disorders report significant symptom relief following therapeutic exercise programs. Various scientific societies focused on the study of headaches and migraines recommend incorporating physical exercise as an integral part of treatment to manage symptoms in these patients. Furthermore, recent evidence supports that a combination of manual therapy and exercise significantly enhances the range of motion and reduces pain intensity in patients with temporomandibular disorders. In the context of migraines, exercise has been shown to positively affect pain frequency, duration, and intensity, as well as disability and quality of life. Experts suggest that exercise prescriptions for migraine patients should be personalized, taking into account the patient's preferences and psychological conditions to prevent potential adverse effects and maximize treatment efficacy. Additionally, treatment models that include therapeutic education can enhance and amplify the effects of exercise programs through a structured approach that includes education about the benefits of exercise, bio-behavioral movement analysis, instruction on movement execution, and goal setting. This is complemented by motivational interviewing techniques to strengthen motivation for change.
Occlusion orthodontics TMD and pain – domain from dentistry or multidisciplinary cooperation?
Prof. Ambra Michelotti BDS, DDS, Hon D, Orth spec, Professor
The relationship between occlusion and temporomandibular disorders represents one of the
major controversies in dentistry. Sound evidence points toward weak and inconsistent associations, between TMD and occlusion. Dentists routinely change dental occlusion, and occlusal changes may also result from a number of TMJ pathologies. A deep understanding of the relationship between occlusion and TMJ problems is crucial for dentists and diagnostic skills to the dental treatment and suggestions on how diagnose and manage TMD are provided. Assess TMJ problems are needed. Furthermore, dentists are also blamed to provoke TMD and for this it is important to know what the effects of the dental treatment on TMJ could be. The condyle fossa relationship is still considered a cause of TMD, but evidence supports that there is a range of acceptable condylar positions and that usually most patients adapt well to changes in this position. This lecture will focus on the most common TMDs occurring before, during or after.
Pediatric maxifacial complex, respiration and posture. Assessment and treatment
Prof. Dr. Mariano Rocabado
Background: The opinion on whether a patient with an anterior open bite should be treated surgically or not is controversial. These patients generally suffer from associated discomfort due to their occlusal instability and musculoskeletal pain.
Clinical Presentation: A 60-year-old woman visited the clinic with dental mobility of her upper
central incisors as her chief complaint. She had a severe anterior open bite, with a history of
continuous grinding and multiple dental restorations in poor condition. Additionally, she
suffered neck pain with movement restrictions.
Conclusion: Dentists can evaluate and treat patients with an anterior open bite using this
integrative model (physical therapy/dentistry) as a possible alternative as part of the treatment for anterior open bite patients.
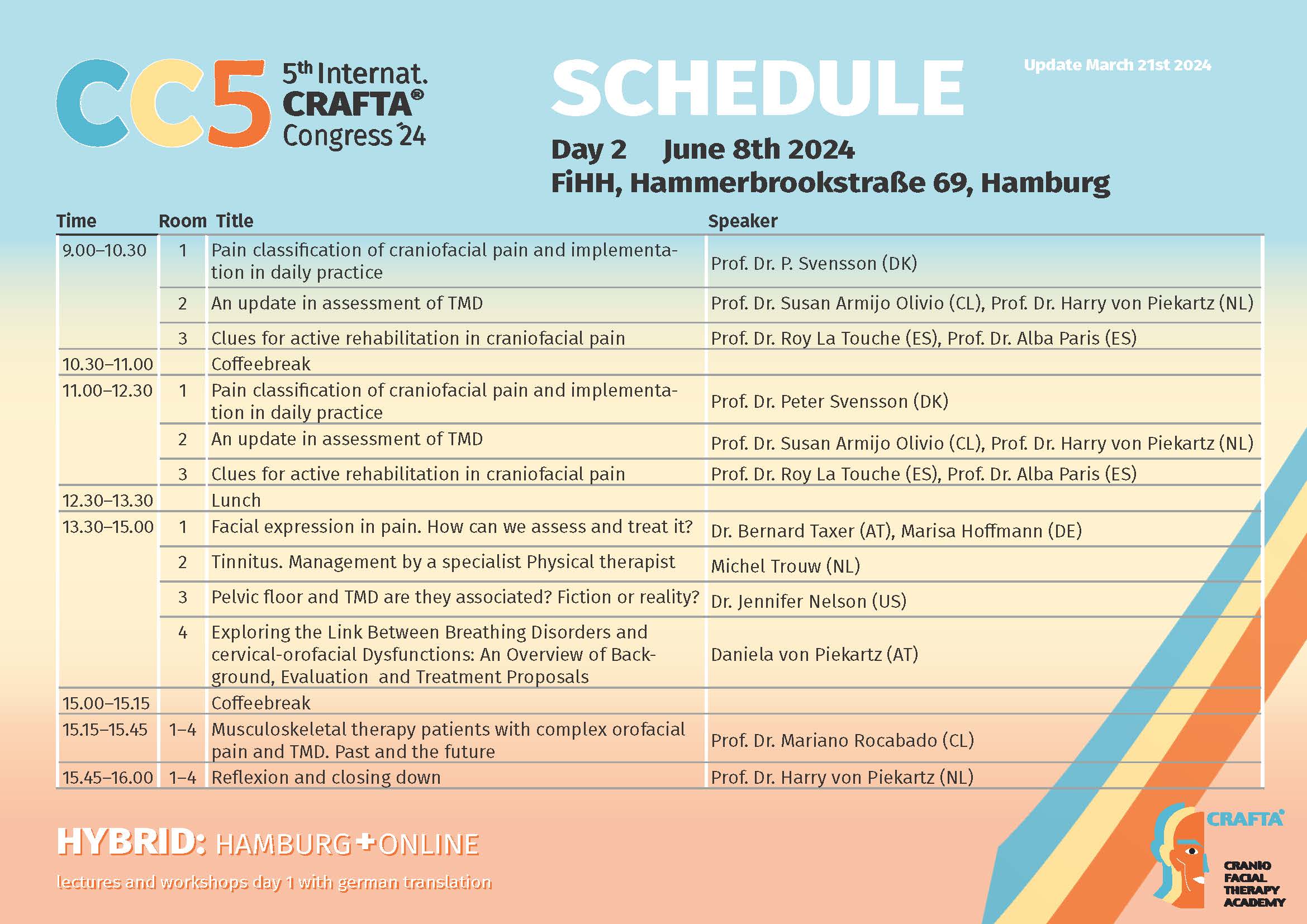
Pain classification of craniofacial pain and implementation in daily practice
Prof. Dr. Peter Svensson, DDS, PhD, Dr.Odont
Classification of pain has greatly developed over the last couple of decades, in particular the recent International Association for the Study of Pain (IASP) and International Classification of Diseases (ICD-11) description of chronic pain as a disease or disorder in its own right (primary pain) is a game changer and clearly note the difference to pain as merely a symptom (secondary pain) (Treede et al. 2019). The International Classification of Headache Disorders (ICHD 2018) is another prominent and important classification system but looks at orofacial pains as secondary headaches attributed to various disorders in specific tissues. Temporomandibular Disorders (TMD) is the second most prevalent orofacial pain condition after odontogenic pains and has progressed substantially with the Research Diagnostic Criteria for TMD (RDC/TMD) (Dworkin and LeResche 1992) and the Diagnostic Criteria for TMD (DC/TMD) (Schiffman et al. 2014). The strengths of these classifications are operationalized criteria and known reproducibility and validity and the international adoption of a common approach to examine and diagnose both painful and non-painful orofacial musculoskeletal disorders. The limitations are obviously the lack of inclusion of other types of orofacial pain but the International Classification of Orofacial Pain (ICOP 2020) attempted to provide a comprehensive classification system of all types of acute and chronic orofacial pain based on the experience from RDC/TMD, DC/TMD, ICHD-3 and IASP-ICD11classifications. The talk will summarize the development of orofacial pain classification with a focus on the need to better integrate neck / cervical pain in future classification systems. This is not just an academic exercise but based on the intimate clinical and neurobiological relationships between some types of orofacial pains and neck / cervical pains leading to the discussion of the term “craniofacial pain” and how to proceed?
An update in assessment of TMD
Prof. Dr. Susan Armijo Olivo, Prof. Dr. Harry von Piekartz
This workshop presents a synthesis of updated assessment and treatment strategies for
Temporomandibular Disorders (TMD), tailored for the continuing education of physiotherapists. It draws from recent advancements in manual and muscular testing methods, integrating these findings into physiotherapeutic practice.
Recent literature has enhanced our understanding of TMD, leading to refined manual testing
procedures that improve diagnostic accuracy regarding joint mechanics and pain responses. Similarly, muscular testing has been advanced to more precisely evaluate muscle coordination and strength, which are vital in differentiating myogenic arthrogenic,neurogenic TMD origins. These updated assessment tools allow physiotherapists to apply more specific and effective interventions.
The treatment of TMD within physiotherapy now emphasizes a multidisciplinary approach. This
includes the integration of manual therapies, tailored exercise regimens, and patient education on self-management techniques such as posture correction,motor control ,systematic (aerobic) training,stress management and Pain Neuroscience Education . Such strategies aim to mitigate symptoms and improve daily functioning in patients with TMD.
The commitment to using evidence-based approaches ensures that physiotherapists are
equipped with the most effective methods for managing TMD. Future directions in research are
expected to focus on the longitudinal efficacy of these strategies and their holistic impact on patient well-being. This workshop underscores the importance of continuous professional development in physiotherapy, promoting an evidence-informed approach to the comprehensive care of TMD.
Clues for active rehabilitation in craniofacial pain
Prof. Dr. Alba Paris-Alemany, MD, PT, PhD
Background: Therapeutic exercise is a well-supported intervention for improving functional capacity and reducing pain in patients with craniofacial pain, including migraines and
temporomandibular disorders. Psychological factors such as catastrophizing and kinesiophobia
can significantly impact the effectiveness of exercise prescriptions in these patients.
Objective: The workshop aims to provide participants with a comprehensive understanding of
the assessment and prescription of therapeutic exercise for craniofacial pain. It focuses on integrating psychological factors into clinical management strategies to enhance treatment outcomes for migraines and temporomandibular disorders.
Methods: The workshop will outline the systematic approach to therapeutic exercise prescription, as defined by La Touche (2020). This involves:
1. Assessment: Using self-report methods to quantify disability and psychological variables (e.g., kinesiophobia, pain catastrophizing) and quantitative measures to
evaluate functional factors such as range of motion, aerobic capacity, and muscle
strength/endurance.
2. Exercise Prescription: Developing a therapeutic plan that includes:
o Local exercises: Targeting craniofacial, mandibular, and cervical regions to
improve mandibular dynamics, neuromuscular efficiency, and load tolerance.
o Global exercises: Moderate-intensity aerobic exercise, yoga, and relaxation training for migraine patients.
o Psychological Interventions: Incorporating graded activity, graded exposure,
motor imagery, and action observation training to address significant psychological factors.
3. Therapeutic Education: Enhancing patient understanding and management of pain through education.
Clinical Relevance: This workshop will enable clinicians to develop robust clinical reasoning
and effective therapeutic strategies for patients with craniofacial pain. By integrating
psychological factors and employing a structured approach to exercise prescription, clinicians
can better manage pain intensity and improve overall patient outcomes. The inclusion of
therapeutic education further supports the effectiveness of therapeutic exercise in this patient
population.
Facial expression of pain: How can we assess and treat it?
Dr. Bernard Taxer, Marisa Hoffmann MSc, BoH, PT, MT (OMPT)
Paul Ekman, widely known for his research in nonverbal communication, described six basic
emotions expressed through the face. Those six emotions – sadness, happiness, disgust, anger,
fear, and surprise – are gender, age, and culturally independent and seem to be important for the so-called facial reflex during nonverbal communication. Research indicates, that facial emotion recognition (FER) is impaired in people with chronic facial pain, somatoform disorders, and low back pain.
Further, recent studies have shown, that pain is also represented in specific patterns in the
face.
FER and pain can be assessed through specific tests. In this presentation we will provide an insight into the current evidence on FER, clinical implications and the practical application. As one example the CRAFTA® training program will be demonstrated.
Tinnitus, Management by a specialist Physical therapist
Michiel Trouw,BSc,MSc PT, MT(OMPT)
This workshop will contain an introduction to the classification systems of tinnitus and the possible position of a specialist Physical therapist. Then we will discuss the CRAFTA examination
and therapy options of the temporomandibular, the cranial, and the cervical region and we will show examples of these techniques and maybe practice some of them.
The final part of this workshop opens the scope to the biopsychosocial context-options in
tinnitus and will show a few examples of the Tinnitus Academyâ approach.
After this workshop participants know what a CRAFTAâ specialist Physical therapist can do in particular tinnitus-patients and what kind of biopsychosocial context can be wise to know about when working with these patient groups.
Chronic hyperventilation, equilibrium and craniofacial dysfunction and pain. Comorbidity, assessment and treatment
Daniela von Piekartz-Doppelhofer , BSc, MSc PT, MT(OMPT), CRAFTA teacher
Hyperventilation syndrome (HVS) is common in patients. It can be a contributing diagnose in
about 10% of general medical patients and up to 25% in patient’s complaining of dizziness or
fainting (Tavel 2021). So therefore, the questions arises if (chronic) hyperventilation syndrome (and other breathing disorders) can be a serious contributing factor for the development and/or
ongoing of craniofacial dysfunctions and pain conditions?
In this workshop we will discuss some important facts about breathing disorders, like background, assessment, and treatment options and how these disorders can affect the
function of the musculoskeletal system and the wellbeing of people.
We also learn if there are contributing factors to this topic which the specialized physical therapist should be aware of and consider in the daily practice.
And we will hear about which dysfunctions and problems are likely to be influenced due to dysfunctional breathing. For example, nek pain (Dareh-Deh et al 2022), postural control disturbances, post-Covid syndrome (Taverne et al 2021), equilibrium disorders, low back pain (Beeckmans et al 2015) and many more.
Dysfunctional breathing can be accompanied by sleep disturbances, change in the brain perfusion, and eventually brain function and therefore lead to cognitive impairment (Friend et al 2019) and even have influence on pain (Jafari et al 2017).
There will be time to practice some of the assessment and treatment options.
The participants of this workshop will not only learn what to do if an acute or chronic
hyperventilation is present but also what the effects can be by changing and normalizing
breathing much more often in patients with craniofacial and other body dysfunctions and pain.
Pelvic floor and TMD, are they associated? Fiction or reality?
Dr. Jennifer M. Nelson DPT, DScPT, FAAOMPT
Learning Outcomes:
-Develop awareness of connections between pelvic floor dysfunction and the Temporomandibular/Craniofacial region. -Gain practical skills in history-taking and clinical examination to assess when treating the pelvic floor for temporomandibular/craniofacial region problems and vice versa could be considered.
Description:
Research in the areas of pelvic floor region and the temporomandibular/craniofacial region have
found connection to the diaphragm, fascia, emotions, and hormones independently. However, little research has looked at the pelvic floor and jaw area together. Furthermore, few clinicians are trained to screen for, or treat problems, in both areas. In this presentation, a case study
will be used to highlight the connection between pelvic floor dysfunction and temporomandibular/craniofacial region problems. Current research about connections between the two areas will be used to make these connections and highlight the areas that need further
research.
Musculoskeletal therapy patients with colpex orofacial pain and TMD. Past and future
Prof. Dr. Mariano Rocabado, PT, MT(OMPT), PhD
The field of musculoskeletal therapy has evolved significantly in its approach to treating
patients with complex orofacial pain and temporomandibular disorders (TMD). Historically, treatments were predominantly focused on symptomatic relief through medications and physical interventions. Early approaches often lacked a comprehensive understanding of the multifaceted nature of orofacial pain, leading to varied outcomes. Recent advancements have emphasized a multidisciplinary approach, integrating dental, medical, and physical therapy perspectives to address underlying causes more effectively. Current research highlights the importance of personalized treatment plans that consider the unique anatomical, physiological, and psychological factors of each patient. Innovative techniques, such as neuromuscular reeducation and advanced manual therapy, have shown promising results in improving patient outcomes. Looking forward, the future of musculoskeletal therapy for TMD and orofacial pain
lies in the continued development of integrative and evidence-based practices. Advances in diagnostic technologies, such as MRI and 3D imaging, are expected to enhance the precision of treatment plans. Additionally, ongoing research into the genetic and molecular bases of these conditions may unlock new therapeutic avenues. Overall, the trajectory of musculoskeletal therapy for TMD and orofacial pain is moving towards more holistic and patient-centered care, promising better management and improved quality of life for affected individuals.

